By Mike Croskery, M.Sc. HK (Biomechanics), Clinical Exercise Physiologist
For years, many knee replacement exercises have focused on 'waking up the quads.' This is often achieved through movements such as squats, leg extensions, and straight-leg raises. Accordingly, there's a good reason for this: studies show that patients who strengthen their quadriceps tend to have better outcomes after surgery (5,14).
However, a strong recovery isn’t just about targeting the quads. Recent research and clinical case studies suggest that the hamstrings (17,18)—specifically, the biceps femoris—also play a crucial role in determining the type of knee replacement exercises chosen. Unfortunately, this approach may often be overlooked and underestimated in rehabilitation.
With hundreds of thousands of knee replacements performed annually (1,3), it's essential to have a comprehensive rehabilitation plan. To help fill this knowledge gap, and from my own perspective as a clinical exercise physiologist specializing in biomechanics with experience working with clients undergoing this procedure, I examined muscle activation in three thigh muscles across three knees that underwent total knee arthroplasty.
The EMG Case Study: Analyzing Muscle Activation Post-Knee Replacement
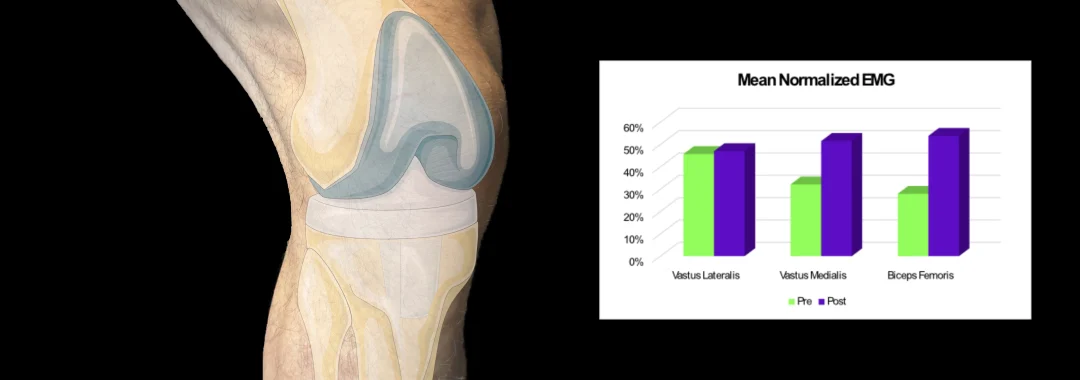
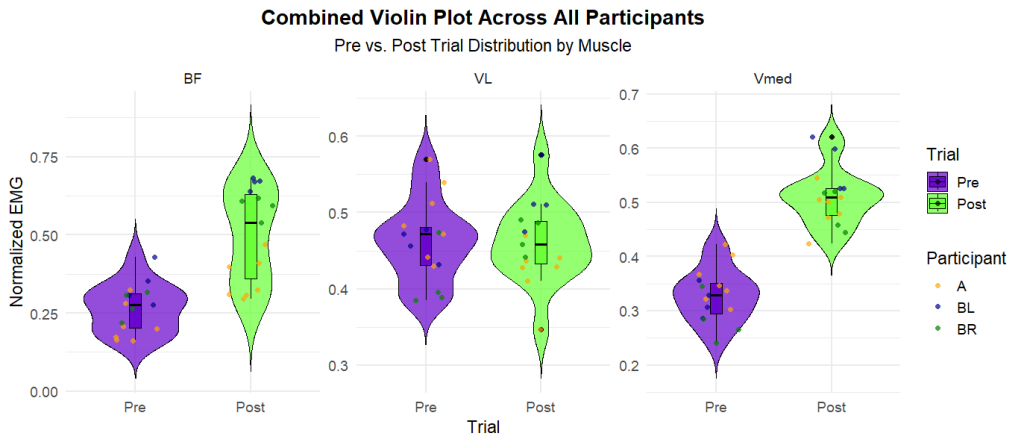
Our study looked at three key muscles in the leg. The vastus lateralis and vastus medialis are located at the front of the thigh, and the biceps femoris is located at the back. What we found was that after knee replacement, both the biceps femoris and vastus medialis were significantly more active than they were before surgery during two knee replacement exercises: the bodyweight squat and step up.
Interestingly, this increased activity might signal a potential compensation or instability issue after surgery. However, understanding why this happens—and what you can do about it—is key to a quicker, more complete recovery. First, let's examine the anatomy of these muscles and understand how they contribute to knee strength.
The Knee Stability Triad: Biceps Femoris, Vastus Medialis, and Vastus Lateralis
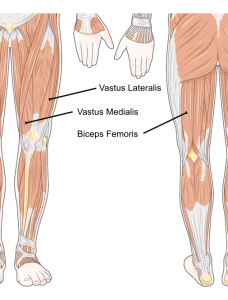
- The biceps femoris (BF) is a major muscle in the hamstring group, and it's located at the back of the thigh. Its main jobs are to bend the knee and extend the hip. It also helps stabilize the lower leg.
- The vastus medialis (VM) is a quadriceps muscle on the inner thigh and is shaped like a teardrop. While its main job is to straighten the knee, it also helps to align and stabilize the kneecap. As a result, several studies have focused on strengthening the VM to help with knee pain (2,4,10).
- The vastus lateralis (VL) is a large muscle on the outer part of the upper thigh. It helps straighten the knee. It also stabilizes both the kneecap and the entire knee joint.
Altogether, these three muscles are fundamental for the force, power, and stability your leg needs.
Normalizing the Data: How We Measured Muscle Response
To understand how muscles recover after surgery, we studied three knees from two patients who underwent total knee replacement. First, we assessed the three muscles before surgery and then again between 3 and 7 months after surgery. All three knees had a normal range of motion at the time of reassessment. However, both patients reported constant pain at the back of the knee during specific knee replacement exercises and movements.
To get a precise understanding of muscle function, we used electromyography (EMG) analysis. The EMG signal measures how your nervous system activates muscles. We looked at muscle activity during four to seven repetitions of two common knee replacement exercises: the bodyweight squat and the step-up.
It's All in the Exercise Comparison
We performed these exercises both pre- and post-knee replacement. Then, we compared the EMG signals to the muscle activity recorded during the step-up. We used the step-up as our benchmark because it isolates each leg, allowing us to focus on individual movements. This provides a more consistent measurement than a squat, which can cause changes in muscle activation between legs due to subtle weight shifts.
Since raw EMG values can differ between people, we "normalized" the data. As such, this scientific process compares the EMG value to a standard. In our case, the standard was the step-up. Normalizing the signal helps us accurately see how hard the muscles are truly working and how the brain is using the muscles' relative capacity. This is then compared to our simple, everyday movement, climbing stairs.
The Hidden Deficit: Why the Hamstrings Struggle After Knee Surgery
Our analysis revealed several interesting findings regarding muscle activation while performing post-knee replacement exercises.
First, the biceps femoris appeared to work significantly harder after surgery to perform the same relative movement. This increase in muscle activation could be due to compensation. It could be behaving this way due to specific muscle weakness or because it is trying to compensate for quadriceps weakness. Because standard rehab often focuses on knee extension, the hamstrings can be overlooked or insufficiently trained. This can leave them weak and overworked.
Second, the vastus medialis also showed higher activity after surgery. Again, this is likely due to the muscle needing to work relatively harder to stabilize the new joint. This finding suggests that a holistic rehab approach is necessary. Likewise, such an approach should not just focus on raw quad strength. It should also focus on the subtle but vital function of the vastus medialis.
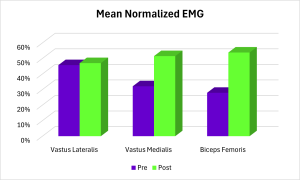
Below, you can see the average muscle response before (purple) and after (green) total knee replacement while performing the knee replacement exercises (squat and step-up).



The EMG Revelation: Comparing Muscle Response in Common Exercises
While averages are helpful, the violin plot below helps us understand the individual differences in the data. Think of it as a heatmap of the data, showing where most results cluster for each muscle before and after surgery.
Interpreting the EMG Data: Effect Size & Confidence
To find a more precise answer, we used a statistical measure known as effect size (7). Effect size helps us determine whether the differences are meaningful in the real-world context of muscle activation during post-knee-replacement exercises.
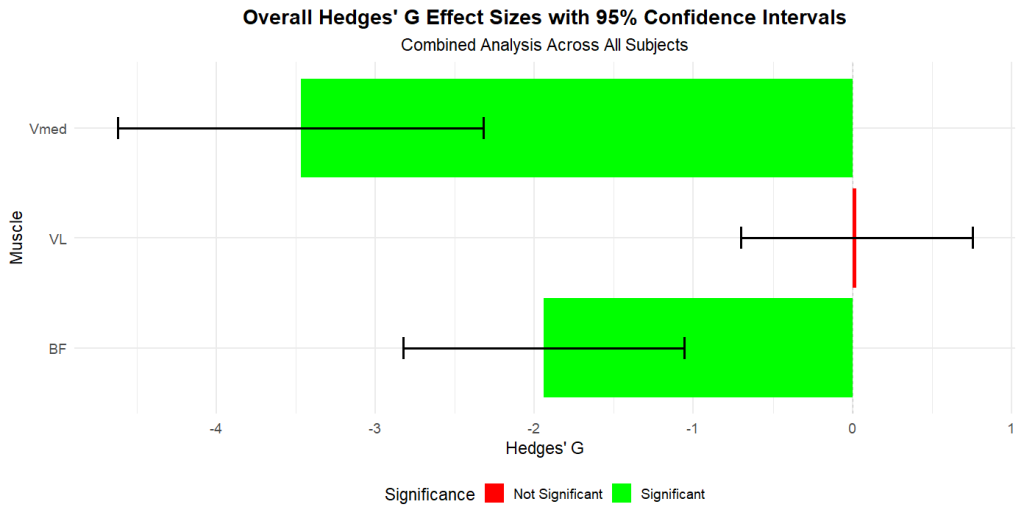
For example, a general guideline for knowing if there are meaningful differences is as follows(16):
- Small: under 0.34
- Large: over 0.65
- Very Large: over 1.2
For both the biceps femoris and vastus medialis, we saw a significant difference in muscle activation. At the same time, the vastus lateralis showed only a minor change. We are also confident that these differences are not due to chance, as the confidence intervals (represented by the black range bars) do not cross the zero line (6).
Important note: Also, keep in mind that these are just three case studies. Individual results are often highly unique to that person. These results may not apply to a larger population.
Clinical Interpretation: Muscle Co-Activation vs. Actual Strength
To understand this, let's review what an EMG signal is and what it is not. EMG measures the signal sent from the brain to the muscle, showing how hard the brain is "telling" the muscle to contract. It does not directly measure strength.
However, the neural signal aligns with the required force. For example, a weaker muscle needs a higher neural signal to create the same force as a stronger one (20).
Therefore, the increased activation we saw suggests these two muscles require a stronger signal after a knee replacement to perform the same movements. The most likely reason is that these muscles have become comparatively weaker after surgery. The structural weakness, combined with a new joint shape and muscle damage, may lead to a less efficient system.
This increased contraction between opposing muscles is called co-activation. After a knee replacement, the nervous system often increases co-activation as a protective response to stabilize the new joint (11,19). This combined opposite muscle contraction is a normal reaction.
However, if a muscle (such as the biceps femoris) is weaker, it will need a stronger signal to help stabilize the joint. Ultimately, this can create imbalances, making a full recovery more difficult.
Phase 1: Your Pre-Surgery Plan ("Prehab")
The first step toward a quick recovery happens before the surgery. As a result, this becomes your pre-surgery plan, also known as "prehab." The goal is clear: to strengthen your leg muscles as much as you can. Accordingly, research supports this approach as it can significantly improve your recovery after surgery (9,21).
Think of it as building a strength "reserve." Having stronger muscles gives you a critical buffer as you begin your recovery.
In this phase, focus on building strength in the front and back of your thighs. Include these knee replacement exercises:
- For your quads: Add exercises like leg extensions, reverse lunges, and leg presses. Be sure to choose movements that don't cause extra pain and that you feel comfortable with.
- For your hamstrings: Include exercises such as hamstring curls or stiff-leg deadlifts. As a result, this will strengthen the back of your legs.
Also, don't forget the rest of your leg! Your calves and hip muscles are crucial to the proper functioning of your legs. Be sure to include them in your routine.
Suggested Routine:
- Beginners: Focus on one or two exercises for the front and back of the thigh. Plan to do 2–3 sets of 10–15 repetitions for each.
- Advanced Lifters: You can increase your workout volume over time. Ultimately, adding more leg exercises and sets to your workout. However, ensure it doesn't worsen any existing knee pain.
Important Tip: You may also want to consult a physiotherapist or exercise specialist to ensure you are on the right track. For more details on designing a workout plan, read the article "Designing a Weight Training Routine."
Phase 2: The Post-Surgery Knee Replacement Exercises ("Rehab")
At first, your rehabilitation phase needs to be guided by a professional. For instance, you will likely receive a list of knee replacement exercises. These will strengthen your quads, hamstrings, and calves. Always follow your healthcare professional's advice on when to start. In the meantime, do not rely only on your pre-op training; consistency is the key to progress.
Once you get the all-clear, it's time to apply what we learned from our case studies. To accelerate your recovery and target those often-overlooked muscles, incorporate these exercises into your routine.
- Start with your hamstrings: Begin your training sessions by focusing on the hamstrings, including the biceps femoris. Rehabilitation exercises, such as various leg curls and stiff-legged deadlifts, can be beneficial for your knee recovery.
-

- Stiff Leg Deadlift

-

- Leg Curl

-

- Seated Elastic Leg Curl

-

- Standing Leg Curl

-

- Single Leg Extension

-

- Leg Extension

")
Learn about how you can assess your risk for ACL injury by examining muscle activation timing...
Concerned about ACL injury risk? This ACL injury risk assessment utilizes advanced technology to help athletes prevent re-injury & return stronger.
ACL Injury Risk Assessment: Prevent Re-injury

Learn about using EMG to select exercises for your biceps...
Our EMG study reveals the best biceps exercises for the long and short heads and how to maximize activation for optimal gains.
Best Biceps Exercises for the Long and Short Heads: An EMG Study

Learn more about assessing knee stability using drop jumps...
Uncover hidden risks in using a drop jump test for ACL recovery. Learn why drop height & pelvis kinematics are crucial to assess return-to-play.
Assessing Readiness: The Hidden Dangers of Drop Jump Tests in Injury Recovery